
Case Report | DOI: https://doi.org/10.3A1579/2578-8868/162
1Department of Neurology, the First Affiliated Hospital of Dalian Medical University, Dalian, Liaoning, China
2Dalian Liguang Rehabilitation Hospital
*Corresponding Author: Ming-Ou Lu, Department of Neurology, the First Affiliated Hospital of Dalian Medical University, Zhongshan Road 222, XiGang District, Dalian, China.
Citation: Duo-Duo Fan., Zhe Wang., Wen-Song Mu., Ming-Ou Lu., (2021) A Case Report of Classical eight-and-a-Half Syndrome and Etiology Analysis. J. Neuroscience and Neurological Surgery. 9(2); DOI:10.31579/2578-8868/162
Copyright: © 2021 Ming-Ou Lu, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 24 February 2021 | Accepted: 19 April 2021 | Published: 26 April 2021
Keywords: eight-and-a-half syndrome; perforator artery; transparent lipid-like changes
Eight-and-a-half syndrome is one-and-a-half syndrome plus ipsilateral seventh (facial) cranial nerve palsy, which was first reported by Eggenberger in 1998. This syndrome is caused by a lesion (most often vascular or demyelinating) in the dorsal tegmentum of the caudal pons. It involves the para pontine reticular formation and the medial longitudinal fasciculus, as well as the nucleus and the fasciculus of the facial nerve. We describe a case of a 56-year-old man presented with eight-and-a-half syndrome. We also discuss the vascular pathology and etiology of this syndrome through the literature review. Most eight-and-a-half syndrome cases are caused by occlusions of the perforating branches of the pons. The pathology can be transparent lipid-like changes at the perforator arteries. It can also be thrombosis at the orifice of the main or perforator arteries. BAH could be a very important factor in perforator artery infarction at the pontine. The etiology is closely related to hyperglycemia. An effective intervention is to avoid bad habits and control the hyperglycemia.
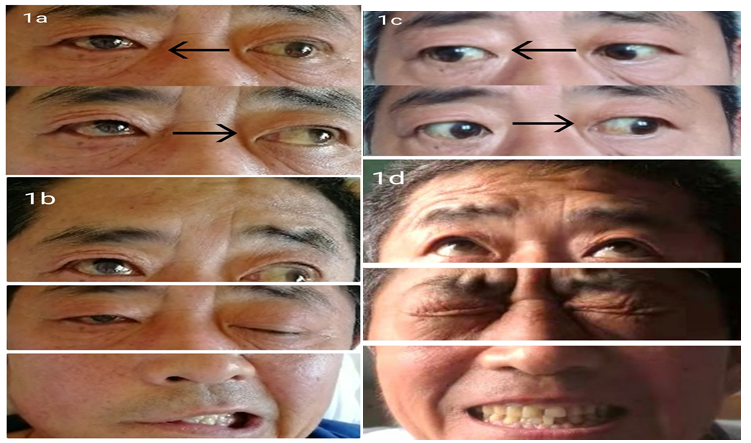
The patient, a 56-year-old male, was admitted to our hospital with the complaint of "sudden dizziness accompanied by blurred vision for one day". His medical history includes hypertension for 5 years (up to 200/120 mmHg), coronary heart disease for 6 years, possible but unconfirmed history of diabetes, smoking (20 cigarettes a day) and alcohol consumption (white spirit 250g a day) for more than 30 years. Physical examination showed BP of 140/75 mmHg, restricted adduction of the left eye, nystagmus when gazing left, restricted abduction, adduction of the right eye and the right eyeball was fixed in the middle. Up- and down-ward movement of both eyes was normal (Figure 1a). His right frontal wrinkles disappeared, right palpebral fissure was larger and right nasolabial folds were shallower (Figure 1b).
Limb strengths were normal. Bilateral Babinski signs were negative. The fasting blood glucose and the glycated hemoglobin were elevated. There was also hyperlipidemia. Head MRI and DWI (diffusion weighted imaging) revealed an acute infarction in the right side of the dorsal pons. MRA (magnetic resonance angiography) showed that the left vertebral artery and internal carotid artery were slightly narrower (Figure 2). Anti-platelet aggregation, blood pressure regulation and lipid regulation were given to stabilize plaque, improve circulation and protect neurons. Symptoms improved after 7 days of treatments. After a month of rehabilitation, the symptoms improved significantly (Figure 1c). The patient was basically normal on the 5th month follow-up. (Figure 1d).

Our patient showed a complete right (ipsilateral) horizontal gaze paresis, partial gaze paresis of the left eye (spared abduction), and right peripheral facial nerve paresis. MRI revealed a right caudal pontine infarction involving the para pontine reticular formation, medial longitudinal fasciculus and VII nerve nucleus. These conformed to the classic eight-and-a-half syndrome.
Studies have shown that most pontine infarctions are caused by transparent lipid-like changes in perforator arteries [5.6]. The pontine perforator artery originates from the basilar artery, and mainly consists of the paramedian branches, the pontine long- and short-circumferential branches. The collateral circulation of these arteries is very poor because they are terminal arteries with small diameters. Also, these arteries are hardly connected to the anterior or posterior cerebral artery [7], so the occlusions of these perforator arteries have almost no compensatory mechanisms.
There are two types of pathological changes in the infarction of perforator arteries: 1) atherosclerosis resulting in thrombosis at the orifice of perforator artery or main artery 2) transparent lipid-like changes leading to arterial wall occlusion. Their clinical treatments and prognosis are different [8]. Based on Figure 2, we suppose that the lesion in our patient is caused by transparent lipid-like changes in the distal part of the long circumferential branches.
A clinical controlled study of 120 patients showed that the etiological factors of most atherosclerotic cerebral infarctions with large arteries were due to alcohol consumption, smoking and abnormal lipid metabolism. However, perforator artery infarction is more related to diabetes mellitus [9]. This is verified by many reported eight-and-a-half syndromes [2.3.4.10.]. Therefore, strict control of blood glucose is an effective preventive measure of perforator artery infarction.
A study of 328 patients with cerebral infarction showed that incidence of basilar artery hypoplasia (BAH) with perforator artery infarction is 8.2%, and it is even higher in the posterior circulation part, especially in pontine perforator artery infarctions [11]. This suggests that BAH may be one of the important vascular causes of pontine perforator artery infarction. This is consistent with the conclusion that congenital arterial hypoplasia usually results in small scattered infarctions [12]. Normally the diameter of the basilar vessel in BAH is evenly smaller (below 2 mm at pontine). The diameter of the basilar artery (pontine level) in our patient is about 2.8mm, which can exclude BAH.
Most eight-and-a-half syndromes are caused by occlusions of the perforating branches of pons. The pathology can be transparent lipid-like changes of the perforator arteries, or thrombosis at the orifice of the main / perforator arteries. BAH could be a very important factor in perforator artery infarction at the pontine. The etiology is closely related to hyperglycemia. An effective intervention is to avoid bad habits and control the hyperglycemia.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
